Heart Failure is creating unsustainable pressure on health systems across Asia-Pacific. A new white paper uncovers where current policy is falling short — with a roadmap to turn the tide.
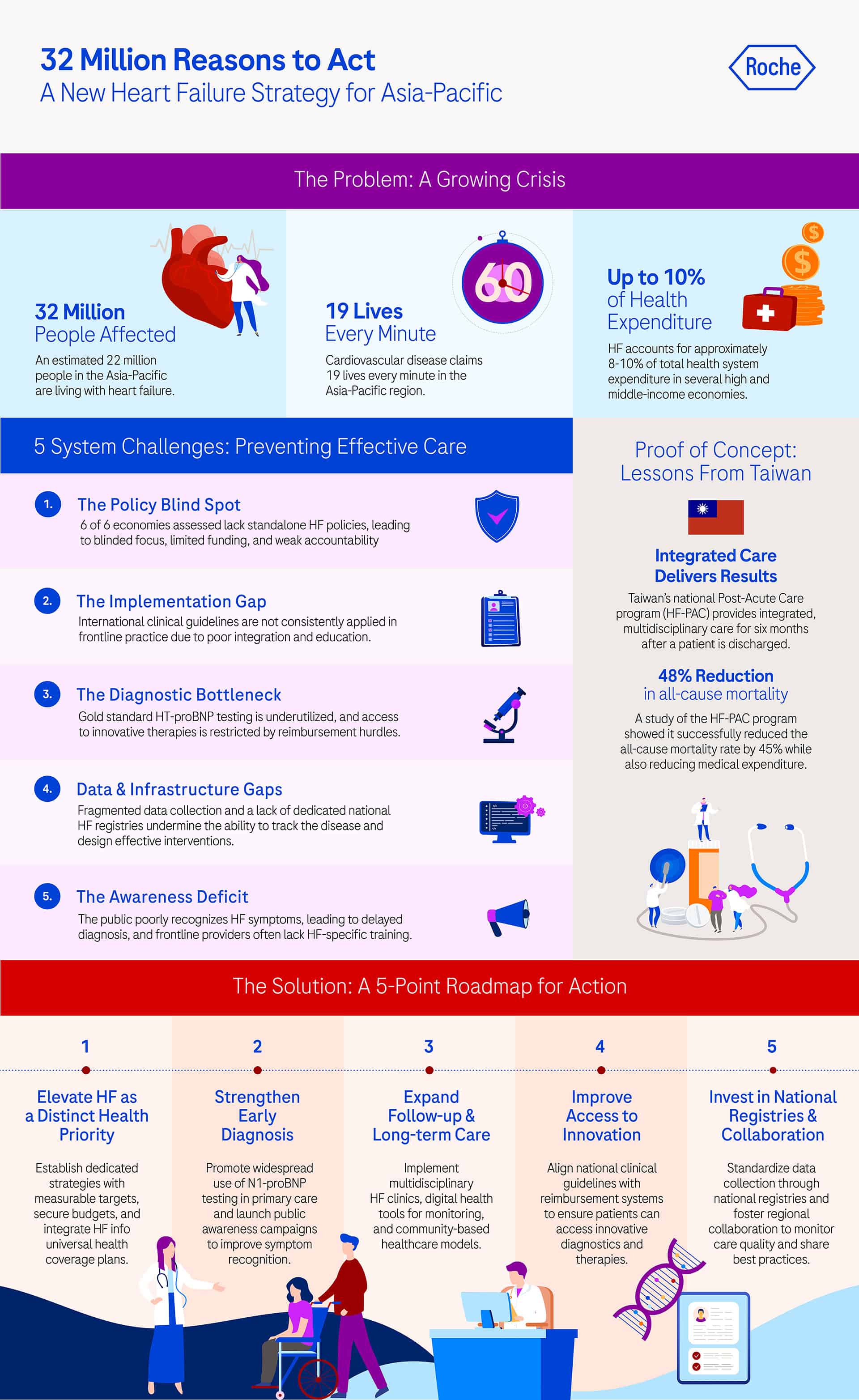
Cardiovascular disease (CVD) — any condition affecting the heart or blood vessels — claims 19 lives every minute in the Asia-Pacific region. But one critical CVD is often overlooked by policymakers: Heart Failure (HF).
Driven by rapidly ageing populations and a surge in comorbidities like hypertension and diabetes, the condition now affects an estimated 32 million people in Asia-Pacific1. HF alone accounts for roughly 8% of health system expenditure in high-income economies such as South Korea, and 10% in middle-income economies such as China and Thailand2.
Yet the warning signs of a growing public health crisis haven’t, so far, led to decisive action. Improving heart failure policy and management in Asia Pacific: Opportunities for impact, a white paper from the APAC CVD Alliance and Deloitte in collaboration with Roche, aims to bridge that gap. It assesses policy approaches to HF in eight Asia-Pacific health systems: Australia, China, Hong Kong, Japan, South Korea, Taiwan, Thailand, and Vietnam.
The white paper serves as a strategic guide for Asia-Pacific governments to drive cost-effective approaches to HF management, improve patient outcomes, and alleviate health system pressure — identifying five system challenges currently preventing effective care.
1. The policy blind spot
The first challenge is visibility. Six of the eight economies assessed lack standalone HF policies or strategies3. In most, HF is subsumed under broader CVD or Non-Communicable Disease (NCD) frameworks.
While this integration is well-intentioned, this leads to diluted focus, limited dedicated funding, and weak accountability mechanisms. Without specific targets or budgets, HF initiatives often fall through the cracks.
2. The implementation gap
Frontline practice is also unaligned with clinical knowledge. While international guidelines such as ESC and AHA have been widely adopted, implementation is inconsistent. Barriers include limited integration of guidelines into primary care, delayed incorporation of new therapies into reimbursement systems, and a lack of continuous professional education4.
3. The diagnostic bottleneck
The third challenge is access to essential tools. The gold-standard tool for early diagnosis, NT-proBNP testing, is underutilised. In many territories, reimbursement barriers restrict the use of NT-proBNP in primary care settings, where patients first present with symptoms.
Innovative therapies, such as SGLT2 inhibitors and ARNI, also face access hurdles due to high costs and slow Health Technology Assessment (HTA) processes.
4. Data and infrastructure gaps
Another major barrier to improvement is data and infrastructure gaps, which currently undermine policy and care quality. HF-related data collection across the Asia-Pacific region is fragmented, with inconsistent coverage and limited interoperability — and few health systems maintain specific HF registries.
Where clinical study or hospital-based registries do exist, they often lack real-world outcomes data and standardised performance metrics. This fragmentation limits leaders’ ability to track the true burden of HF, evaluate the quality of care, or design evidence-based interventions.
5. The awareness deficit
Finally, HF symptoms are poorly recognised among the general public, particularly within elderly and rural populations. This directly contributes to delays in care access and diagnosis. Community health education programmes are rare outside of high-income settings.
Simultaneously, frontline providers face significant gaps in HF-specific training, particularly regarding the application of diagnostics and the initiation of Guideline-Directed Medical Therapy (GDMT) in community settings.
Lessons from regional leaders
Despite these challenges, progress is possible. Two economies in particular have already demonstrated the potential policy-driven interventions to improve outcomes.
Taiwan
In Taiwan, a national HF Post-Acute Care (HF-PAC) embeds integrated HF care within the National Health Insurance system, allowing for joined-up multidisciplinary care from predischarge to ambulatory care for six months after discharge5.
Patients who have been hospitalised for acute or decompensated chronic HF (patient status: American College of Cardiology Foundation/American Heart Association stages C or D), had a left ventricular ejection fraction (LVEF) of ≤40%, and were discharged following hospitalisation and aged 18 years or older are eligible to be enrolled.
A nationwide propensity score-matched study (October 2017 – March 2021) shows the HF-PAC programme’s success: all-cause mortality rate was reduced by 48% during a mean follow-up of 1.59 years6, with reduced medical expenditure.
Japan
In Japan, deaths from HF are rising. Around 1.2 million HF patients were diagnosed in 2020 with a projected peak of 1.32 million in 2035, attributed to a rapidly ageing population. The costs of cardiovascular disease are higher in Japan than any other condition; among the population aged 65+, expenditure is even higher — possibly related to length of hospital stay.
Preventing re-hospitalisation is therefore key. Yet GDMT doesn’t currently meet this need, particularly in outpatient clinics. Early detection and prevention of HF with regular surveillance using BNP/NT-proBNP-guided HF therapy must be top priority for health system leaders.
Plotting the roadmap for action
These case studies show that we can begin to tackle the growing burden of HF in the region — with the right policy approach. The white paper translates insights into action with key recommendations including:
- Elevating HF as a distinct health priority with dedicated budgets, strategies with measurable targets, and integration into universal health coverage plans.
- Strengthening early diagnosis through greater use of NT-proBNP testing, across primary and tertiary care, alongside public awareness campaigns to enhance symptom recognition.
- Expanding follow-up and long-term care via multidisciplinary HF clinics, digital health tools, and community-based workforce models.
- Improving access to innovative diagnostics and therapies by aligning clinical guidelines with reimbursement systems.
- Investing in national HF registries and regional collaboration to standardise data, improve monitoring, and share best practices.
The burden of heart failure weighs more heavily on Asia-Pacific health systems than almost any other condition — but hope is not lost. The path forward is clear. We have the tools, the clinical insight and the regional blueprint to address this challenge. What must follow now is action.
Over 20 clinical experts kindly gave up their time in the production of this white paper. Now, we’re asking for one more thing — from you. Please like, share or repost this article, so we can give HF patients a louder voice. You may access and download the white paper here to learn more. Thank you.