Note: This article was adapted from an opinion editorial article written by Dr. dr. Dewi Wulandari, M.Sc, Sp.PK(K), Head of the Immunology and Biomolecular Division, Clinical Pathology Department, Faculty of Medicine, Universitas Indonesia. The article was published on The Jakarta Post, “Can Our Labs Achieve Cervical Cancer Screening Targets” on 24 December 2025. The original article can be accessed here.
Cervical cancer is one of the most preventable forms of cancer, yet it remains among the most underdetected and deadly for women in Indonesia. This gap is not due to a lack of medical knowledge or technology. Rather, it reflects a system-level challenge in the design, delivery, and scaling of screening services to reach women effectively.
Cervical cancer is one of the most preventable forms of cancer, yet it remains among the most underdetected and deadly for women in Indonesia. This gap is not due to a lack of medical knowledge or technology. Rather, it reflects a system-level challenge in the design, delivery, and scaling of screening services to reach women effectively.
Indonesia has taken an important step by adopting HPV DNA testing as the primary method for cervical cancer screening, in line with World Health Organization (WHO) recommendations. However, policy adoption alone does not guarantee impact. Screening programs are only as effective as the systems that support them—particularly laboratory readiness, logistics, workforce capacity, and quality assurance.
From Policy Adoption to Operational Readiness
A central challenge lies in translating screening intent into operational capability. While HPV DNA testing is part of the national strategy, laboratory capacity to process PCR-based tests remains uneven across the country. Without sufficient and reliable testing capacity, samples collected from women cannot consistently be converted into timely and accurate results. When this happens, trust in the screening program is weakened, and participation suffers.
At the same time, Indonesia may be more prepared than it appears. The COVID-19 pandemic has accelerated a rapid expansion of molecular testing infrastructure nationwide. PCR machines were deployed, laboratory facilities strengthened, and thousands of laboratory analysts trained. Much of this capacity remains available today. The challenge, therefore, is not access to technology, but the effective redeployment and coordination of existing resources.

Lab technician operates the automated molecular diagnostics system cobas 5800
One practical approach to addressing this challenge is the hub-and-spoke laboratory model. Under this system, high-capacity laboratories in urban centers serve as testing hubs, while primary care facilities and community-based health posts act as spokes focused on sample collection. Samples are transported from spokes to hubs for processing, allowing the health system to maximize existing laboratory investments while extending reach to underserved populations.


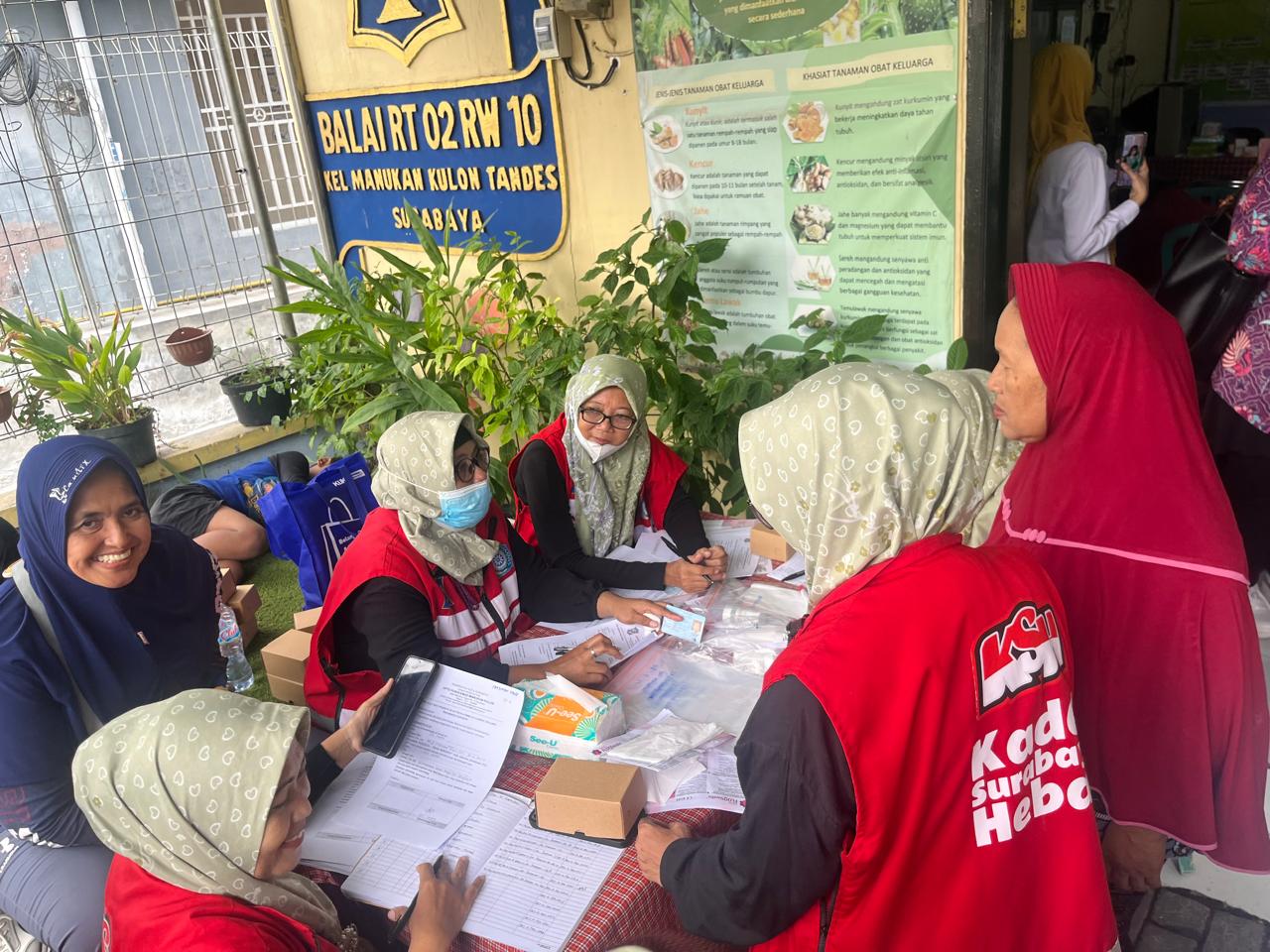
Hub-and-Spoke Pilot Project Implementation in East Java
“This HPV DNA screening program is highly beneficial for the community, helping women understand their HPV infection status. This was my first experience screening cervical cancer, and I initially felt afraid and embarrassed; however, the self-sampling collection was not painful at all. I encourage all women to never hesitate or feel ashamed to take part in HPV DNA screening whenever the opportunity arises—for our own health,” said Siti Hani, one of the women cadres in Surabaya.
Infrastructure alone is not enough. People and processes determine whether screening programs succeed. Health workers play a critical role—not only in facilitating sample collection and referrals, but also in building trust through clear, empathetic communication. Self-sampling can reduce barriers related to access, stigma, and discomfort, but only if women understand and trust the process.
As screening expands, quality and consistency become essential. Variability in testing performance can undermine confidence and threaten long-term adoption. In recent years, the diagnostic landscape has seen an influx of locally available reagents, underscoring the importance of rigorous validation and quality assurance. In a country where HPV genotype distribution may differ from global averages, screening programs must rely on assays that are thoroughly evaluated and aligned with international standards. For women to trust the system, they must trust the test.
Meeting national and global targets for cervical cancer elimination by 2030 requires laboratory readiness to be treated as a core pillar of the screening strategy. This means redeploying trained personnel, reactivating underused laboratories, investing in validated diagnostic tools, and strengthening referral and follow-up pathways. Integration with broader digital health initiatives, such as Satu Sehat, and alignment of sustainable financing mechanisms will be essential to support scale.
Moving Forward
Indonesia has the tools, infrastructure, and expertise needed to deliver effective cervical cancer screening. The experience of recent years has shown that rapid system transformation is possible when resources are aligned and coordinated. By reactivating existing capacity, optimizing delivery models, and building trust at the community level, screening programs can move from fragmented efforts to sustained national impact. No woman should die from a cancer that can be detected early and prevented.