What if a new approach to testing could identify people living with a deadly disease that begins with no symptoms?
Hepatitis B virus (HBV) is hard to catch early. There are typically no symptoms until the disease has progressed well beyond early stage and serious complications like liver fibrosis, cirrhosis, and Hepatocellular Carcinoma (HCC) have arisen; life expectancy for an advanced stage diagnosis is just 7—22 months1.
That makes HCC one of the most difficult public health challenges facing the Asia-Pacific region’s health systems. Early detection is vital to save lives. Yet while the diagnostics that can detect chronic disease influence up to 70% of clinical decisions, they’re widely underrecognised, receiving just 2% of funding2.
As a result, HBV and other chronic diseases are often caught too late — at enormous cost to the individuals, and the health systems that serve the
New Zealand’s vision for change
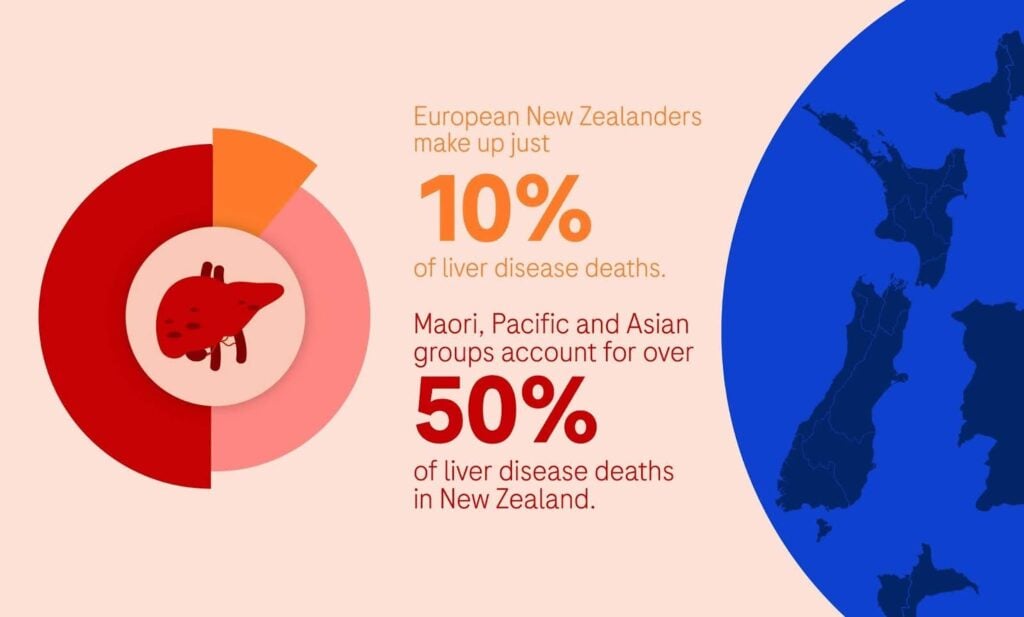
New Zealand’s National Hepatitis B Screening Programme (NHBSP) gives us the blueprint for a more proactive approach. In New Zealand, Māori, Pacific peoples, and Asian communities are disproportionately affected by HBV, representing over 50% of liver disease mortality compared to 10% among European New Zealanders3.
The programme aims to meet these groups where they are, shifting the focus from late-stage emergency intervention to structured, early surveillance to transform liver cancer outcomes.
GAAD tests — which integrate advanced serum biomarkers like PIVKA-II alongside alpha-feto protein (AFP) tests into the Standard of Care (SOC) — are provided via blood tests at local clinics, giving clinicians the answers they need early while significantly reducing the systemic demand for specialised imaging services.
Patients are actively managed through a formal registry, moving away from a reactive “test-and-treat” model toward a “monitor-and-prevent” framework. This model — unique for being government-funded yet executed by the expert NGO, The Hepatitis Foundation of New Zealand — has successfully closed the diagnosis gap.
By screening 177,292 people, the initiative has identified 11,936 individuals with chronic HBV, transitioning them into a life-saving framework of biannual monitoring and lifelong follow-up.
Equitable access to screening saves lives
Key to this success was a commitment to equitable access. The programme spotlighted the disproportionate impact of HBV on Māori and Pacific Islander communities. By securing the local leaders’ endorsement, the programme tackles stigma at the grassroots level, turning a medical intervention into a proactive community health solution.
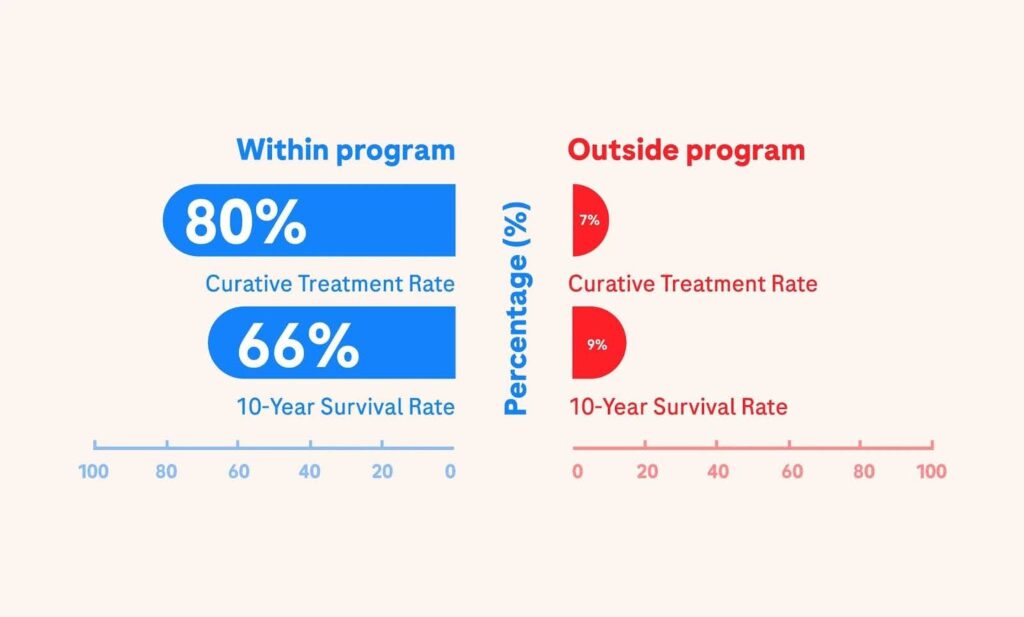
And for those who have been diagnosed, the clinical outcomes are transformative. 80% of HBV-HCC cases have been detected early enough for curative treatment, compared to a mere 7% curative rate for those diagnosed outside the program1 — increasing the 10-year survival rate for those diagnosed within the program from 9% to 66%.
The program now manages over 16,000 individuals, drastically shifting the trajectory of the disease. Palliative cases have dropped from 68% in 1996 to 26% in 20211. Significant progress has been made in preventing mother-to-child transmission4.
Time to end the postcode lottery
The programme’s success proves that early detection saves lives — but there’s a long way yet to go. Obesity and diabetes are driving widespread prevalence of metabolic dysfunction-associated fatty liver disease (MAFLD). Liver cancer is still a heavy burden on New Zealand’s health system.
Clinicians still largely rely on six monthly alpha-feto protein (AFP) tests and ultrasounds to screen high risk patients; demand is high and these tests are often unable to detect HCC in patients with advanced fatty liver and NASH5. Rising HCC in NASH patients without cirrhosis complicates screening decisions5.
Care delivery, meanwhile, is hindered by low GP engagement and high mistrust, particularly among the Māori. A strict ‘did-not-attend’ policy requires patients to secure new referrals if they miss an appointment. This creates a systematic barrier that disproportionately affects communities who have difficulty navigating the healthcare system, leading to a postcode lottery of care.
The roadmap for success
These outcomes show that to turn the tide on liver disease, we must ensure all communities can access life-saving screening — regardless of where they live. To rebalance health inequities, particularly for rural and underserved Māori and Pasifika populations, healthcare must meet patients where they are, ensuring that geographic location doesn’t dictate survival.
This means:
- Scaling collaboratively. The programme shows how public-private partnerships can successfully expand testing reach and improve access to care.
- Providing access to advanced diagnostics. Integrating serum biomarkers like PIVKA-II with AFP into the Standard of Care (SOC) enables blood-based triaging in community health settings rather than requiring a visit to an urban hospital.
- Prioritising equitable access. Recognising that one size doesn’t fit all improves access for Māori, Asian, and Pacific Island communities. Targeted awareness campaigns and free screening can improve engagement and overcome traditional barriers to care.
- Improving outreach strategically. By adopting proven engagement strategies from a successful Hepatitis C prevention campaign, we can reach more of the high-risk population for HBV and normalise proactive screening.
Replicating New Zealand’s success
The postcode lottery of HBV care is a solvable problem. By decentralising diagnostics with serum biomarkers and point-of-care testing, we can decouple survival from geography.
The mission is clear: we must build a system that prioritises lifelong survival over late-stage treatment. We have the roadmap; now we must replicate New Zealand’s success. It’s the only way to give people living with HBV more time with their families.
If this article resonates with you, please help us to raise awareness of the need for early detection of HBV — by liking, commenting or reposting. Thank you.